Drugs that Affect the Autonomic System
Objectives:
By the end of this section, you will be able to:
- List the classes of pharmaceuticals that interact with the autonomic nervous system
- Differentiate between cholinergic and adrenergic compounds
- Differentiate between sympathomimetic and sympatholytic drugs
- Relate the consequences of nicotine abuse with respect to autonomic control of the cardiovascular system
An important way to understand the effects of native neurochemicals in the autonomic system is in considering the effects of pharmaceutical drugs. This can be considered in terms of how drugs change autonomic function. These effects will primarily be based on how drugs act at the receptors of the autonomic system neurochemistry. The signaling molecules of the nervous system interact with proteins in the cell membranes of various target cells. In fact, no effect can be attributed to just the signaling molecules themselves without considering the receptors. A chemical that the body produces to interact with those receptors is called an endogenous chemical, whereas a chemical introduced to the system from outside is an exogenous chemical. Exogenous chemicals may be of a natural origin, such as a plant extract, or they may be synthetically produced in a pharmaceutical laboratory.
Broad Autonomic Effects
One important drug that affects the autonomic system broadly is not a pharmaceutical therapeutic agent associated with the system. This drug is nicotine. The effects of nicotine on the autonomic nervous system are important in considering the role smoking can play in health.
All ganglionic neurons of the autonomic system, in both sympathetic and parasympathetic ganglia, are activated by ACh released from preganglionic fibers. The ACh receptors on these neurons are of the nicotinic type, meaning that they are ligand-gated ion channels. When the neurotransmitter released from the preganglionic fiber binds to the receptor protein, a channel opens to allow positive ions to cross the cell membrane. The result is depolarization of the ganglia. Nicotine acts as an ACh analog at these synapses, so when someone takes in the drug, it binds to these ACh receptors and activates the ganglionic neurons, causing them to depolarize.
Ganglia of both divisions are activated equally by the drug. For many target organs in the body, this results in no net change. The competing inputs to the system cancel each other out and nothing significant happens. For example, the sympathetic system will cause sphincters in the digestive tract to contract, limiting digestive propulsion, but the parasympathetic system will cause the contraction of other muscles in the digestive tract, which will try to push the contents of the digestive system along. The end result is that the food does not really move along and the digestive system has not appreciably changed.
The system in which this can be problematic is in the cardiovascular system, which is why smoking is a risk factor for cardiovascular disease. First, there is no significant parasympathetic regulation of blood pressure. Only a limited number of blood vessels are affected by parasympathetic input, so nicotine will preferentially cause the vascular tone to become more sympathetic, which means blood pressure will be increased. Second, the autonomic control of the heart is special. Unlike skeletal or smooth muscles, cardiac muscle is intrinsically active, meaning that it generates its own action potentials. The autonomic system does not cause the heart to beat, it just speeds it up (sympathetic) or slows it down (parasympathetic). The mechanisms for this are not mutually exclusive, so the heart receives conflicting signals, and the rhythm of the heart can be affected.
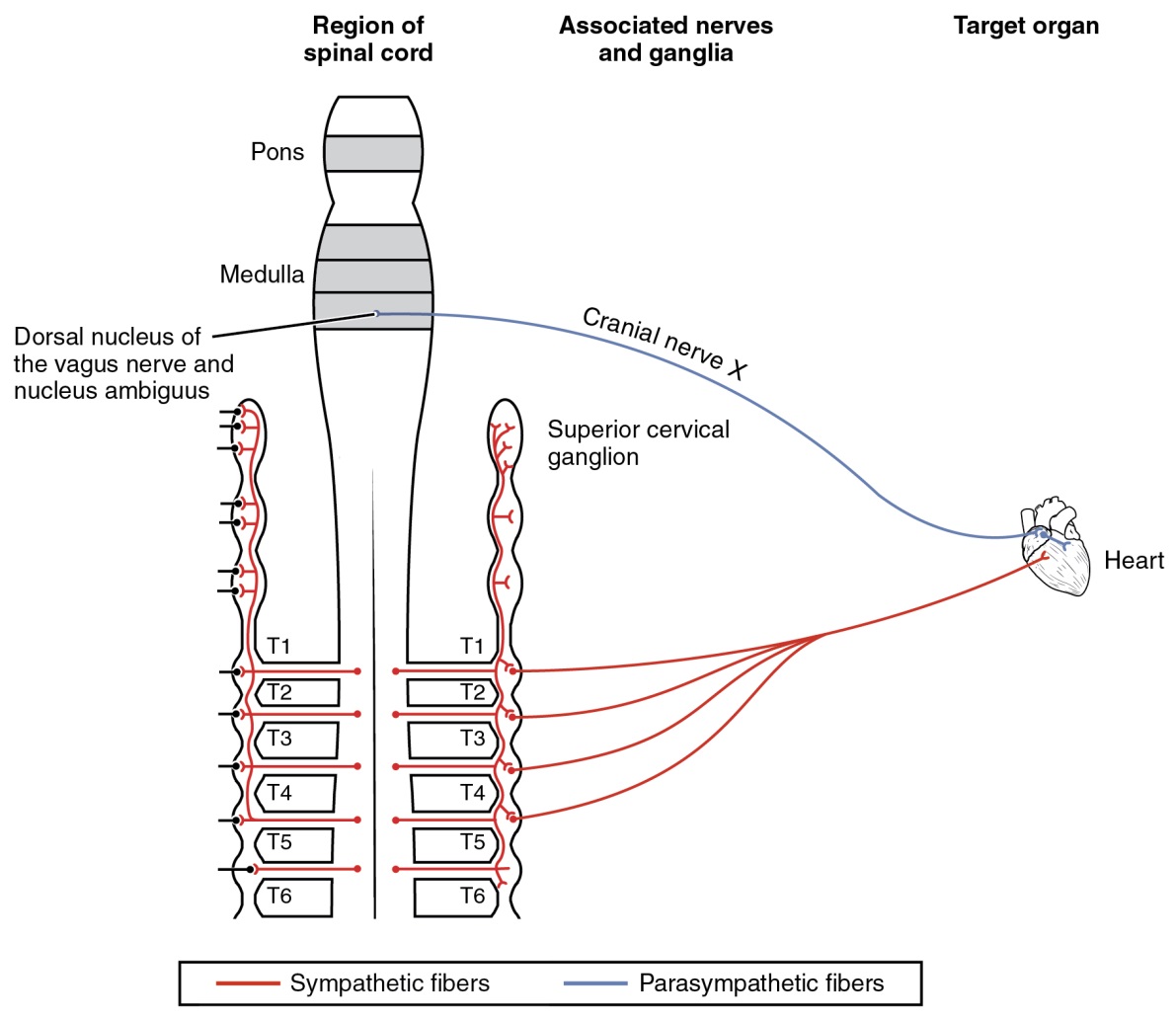
Figure 9: The nicotinic receptor is found on all autonomic ganglia, but the cardiovascular connections are particular, and do not conform to the usual competitive projections that would just cancel each other out when stimulated by nicotine. The opposing signals to the heart would both depolarize and hyperpolarize the heart cells that establish the rhythm of the heartbeat, likely causing arrhythmia. Only the sympathetic system governs systemic blood pressure so nicotine would cause an increase.